
Last updated on December 28th, 2023
In this post, we’ll discuss the lithotomy position in detail. We’ll discuss its definition, indication, procedure, variations, and complications.
What is lithotomy position?
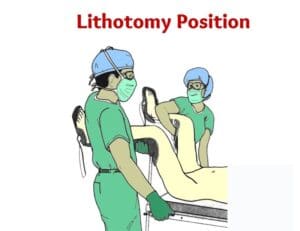
The lithotomy position is one of the many variations of dorsal or supine positions. It involves patient positioning on his/her back with both the legs elevated and rested on an assistive device called stirrups.
Nurses position the patient in the lithotomy position in preparation for gynecologic, obstetric, urologic, and proctologic examinations and surgeries. It offers maximal exposure of genitalia hence facilitating easy access to the perineal exams and procedures. It is also commonly used position for childbirth like Sims’ position.
Lithotomy position by itself has different variations. They are low, standard, high, exaggerated, and hemi lithotomy positions. Also, there is a modified version known as the dorsal lithotomy position.
Another similar dorsal position is the dorsal recumbent position. Click here to learn the difference between lithotomy position and dorsal recumbent position.
History of Lithotomy
The origin of the term lithotomy goes back to 207 BC and it was coined by an Alexandrian lithotomist Ammonius Lithotomos. Moreover, the Greek term ‘litho’ literally means ‘stone’ and ‘tomos’ means ‘cutting’. Hence, the procedure of cutting of calcui is called ‘lithotomy’.
Also, the reference to lithotomy is found in Hippocrates oath as well. “I will not cut for the stone, but will leave this to be done by practitioners of this work…”
It is recorded that, historically lithotomists performed the procedure by keeping the patient in the lithotomy position.
Mainly five methods of lithotomy were used historically. Namely,
- The Celsian, or ‘lesser operation’
- The Marian, or ‘greater operation’
- The lateral operation
- Suprapubic cystotomy, or ‘high operation’
- Cutting through the rectum or proctocystotomy
Each of these methods has evolved with the advancement of surgical techniques and technology.
Definition
Lithotomy position can be defined as a supine reclining posture with legs elevated with support of either candy cane, knee crutch, or boot support.
How to place patient in lithotomy position?
The procedure for lithotomy positioning the patient is as follows.
- Keep the patient in supine position on the OR table
- Fix the stirrups which is going to be used to support legs during the procedure.
- Move the patient down to the lower edge of the OR table. Ensure buttocks of the patient is not hanging over the edge of OR table.
- Then, both legs are simultaneously put in the stirrups by two person – one for each leg. This step should be performed slowly and smoothly.
- Remove the foot-end of the OR table
- Adjust height and position of the stirrups as per the procedure. Also, ensure both the stirrups are at equal heights.
- Keep the arms either on arm-boards or tucked at patient’s side as per the procedure.
- At the end of the procedure, the legs and feet are released simultaneously in a controlled manner by two people supporting each leg.
- Lower peripheral pulses are checked and documented before, during, and after positioning the patient.
Indication for Lithotomy Position
Some of the indications for lithotomy position are as follows.
- Gynecologic pelvic examination to determine cervical dilation during labor – mostly uses the standard lithotomy position
- Urologic examination of the prostate gland (digital rectal exam) – uses the low lithotomy position.
- Colorectal surgical procedures such as left colectomy and sigmoid colectomy
- Urologic surgical procedures such as perineal prostatectomy and transrectal prostate biopsy.
- Childbirth
- Pelvic procedures such as ureteroscopy and hysterectomy.
- Urologic transurethral resection of the bladder or prostate tumors
- Other surgeries of male urethra
Risks Factors
- High BMI
- Blood loss
- Peripheral vascular disease
- Hypotension
- Reduced cardiac output
Types of Lithotomy Position
There are different variations of lithotomy position. These are classified based on how high the patient’s lower extremities are elevated for the procedure.
The types of lithotomy positions include the following.
- low lithotomy position,
- standard lithotomy position,
- high lithotomy position,
- exaggerated lithotomy position, and
- hemi lithotomy position
Low Lithotomy Position
The low lithotomy position is most commonly used for urologic procedures. It is also used for other surgical procedures which need simultaneous access to the perineum and abdomen.
In low lithotomy position, you flex the patient’s hip until the angle between the posterior surface of the patient’s thighs and the OR bed surface are approximately 30 to 45 degrees. The patient’s lower legs are parallel with the OR bed.
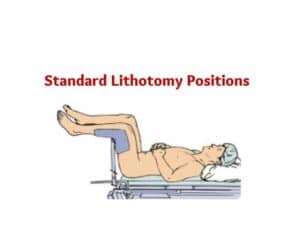
Standard Lithotomy Position
The standard lithotomy position is most commonly used during gynecologic and obstetric exams and procedures. This position is commonly used during childbirth as well.
To position the patient in standard lithotomy position, you flex the patient’s hips until the angle between the posterior surface of the patient’s thighs and the OR bed surface are approximately 80 to 100 degrees. The patient’s lower legs are parallel with the OR bed.
Click here to learn more about Sims’ Position
High Lithotomy Position
High lithotomy position is used when the surgeon requires enhanced perineal access for the procedure.
In high lithotomy position, you place the patient’s hips flexed until the angle between the posterior surface of the patient’s thighs and the OR bed surface are approximately 110 to 120 degrees. The patient’s lower legs are flexed.
Exaggerated Lithotomy Position
The exaggerated lithotomy position is usually used when the surgeon needs transperineal access to the retropubic area. This extreme position helps to move the patient’s legs completely out of the way of the surgical field.
A study reports that general anesthesia (GA) poses significant respiratory and arterial oxygenation risks to patients in the exaggerated lithotomy position. Therefore, you should be extra cautious while monitoring patients in this position with GA.
To position the patient in exaggerated lithotomy position, you flex the patient’s hips until the angle between the posterior surface of the patient’s thighs and the OR bed surface are approximately 130 – 150 degrees and propped upward on a pillow or pad. The patient’s lower legs are almost vertical.
Hemi-lithotomy Position
As the name suggests hemi-lithotomy position is used when one leg is put in lithotomy position while the other leg is extended for the surgical procedure. The hemi-lithotomy position is sometimes used in orthopedic surgeries related to femur fracture.
To position the patient in hemi-lithotomy position, you place the patient’s non-operative leg in a standard lithotomy position with stirrups. Then, the patient’s operative leg can be placed in traction.
Modified Dorsal Lithotomy Position
The dorsal lithotomy position is a modified version of the lithotomy position. Basically, modified dorsal lithotomy position means, putting the patient in either Trendelenburg position or reverse Trendelenburg position while the patient is still remaining in the lithotomy position (i.e., lithotomy position plus Trendelenburg position or reverse Trendelenburg position).
Dorsal lithotomy position with Trendelenburg position pushes internal abdominal structures downwards. While dorsal lithotomy position with reverse Trendelenburg position pushes internal abdominal structures upwards. These positions facilitate easier access and more room for the surgeon to operate.
Click here to learn the difference between lithotomy position and dorsal recumbent position.
Equipment used for lithotomy position and its risks
Various types of stirrups are the main devices used in the lithotomy positions.
The most commonly used types are candy cane-shaped bars with straps, knee crutches, and boot-type stirrups. Each device has its own risks. Hence, you should be aware of the risks associated with each device.
The straps of candy cane-shaped bars are wrapped around the ankles and plantar surface of the foot. It can put pressure on the common peroneal nerve causing footdrop and lack of sensation below the knee.
While knee crutch stirrups keep weight of the leg rests solely on the knee supports. This can put excessive pressure on the posterior tibial and common peroneal nerves, and the popliteal artery. Which may result in complications such as compartment syndrome and peripheral neuropathies.
The boot-type stirrups are boot-like devices which support the lower foot, heel, and up to the midcalf area. It allows controlled and limited abduction while supporting the foot and calf at once. Which allows distributing pressure more evenly.
Thereby, reducing the risk of extreme localized compression on any single area of the foot or leg. However, you must ensure proper positioning of the foot and leg in it.
Contraindications of Lithotomy Position
The lithotomy position is contraindicated in the following:
- Diminished lung capacity
- Pressure injuries
- Muscle injuries
- Hip dislocation
- Preexisting nerve injuries
Complications of lithotomy position
Lower extremity neuropathies and compartment syndrome are the main complications associated with lithotomy position.
Compartment syndrome is rare and it occurs as a result of prolonged surgeries usually more than 2 to 3 hours.
Usually, lower extremity neuropathies occur due to prolonged and/or inappropriate lithotomy positioning during surgeries or childbirth.
Symptoms of lower extremity neuropathies become apparent within few hours after surgery. Symptoms may include footdrop, ankle aversion, and loss of sensation.
Lithotomy position and nerve injury
The most commonly injured nerve due to lithotomy positioning is the common peroneal nerve. Compression behind the knee can cause common peroneal nerve and tibial nerve damage. Symptoms of this nerve damage include foot inversion, foot drop, and loss of sensation in the lower leg.
Other peripheral neuropathies of lithotomy position involve sciatic nerve, femoral nerve or lumbosacral plexus, and obturator nerve.
Injury to these nerves occurs due to a prolonged procedure or improper lithotomy positioning such as hyperflexion.
How to assess the integrity of these nerves?
Following are the ways to assess nerve integrity.
- If the patient is able to dorsiflex the great toe (point it upward) means an intact common peroneal nerve.
- If the tibial nerve is intact, patient will be able to feel his/her normal sensation at the plantar surface of the foot and can curl the toes downwards.
- If the patient is able to bend the thigh typically means the sciatic nerve is intact.
- If the patient is able to adduct the leg normally means an intact obturator nerve.
- If the patient is able to move the thigh to the trunk usually means the femoral nerve is intact.
Preventive Measures
Surgical team must take appropriate preventive measures to protect the patient from nerve injuries related to lithotomy positioning.
Following are important points to remember when you place the patient in the lithotomy position.
- Ensure safety of the stirrups before transferring patient to the OR table. Any malfunction of these devices can cause hip dislocation, muscle or nerve injury, or bone fractures.
- Confirm that the lateral head of the fibula does not rest against stirrup bars or any other hard surface.
- Avoid hyperabduction of the hips during positioning.
- Once patient is in position, ensure stirrups are used in a way that distribute support and pressure over a large area of the patient’s back and legs.
- No pressure should be placed on the legs from stirrup edges or leaning surgical staff.
- Ensure the knees are not bend beyond 90 degrees, even if the hip is flexed beyond 90 degrees.
- Try to minimize the amount of time in lithotomy position as much as possible. If it takes more than 2 hours, you may consider using compression stockings/IPCDs.
- Ensure compressive leg wraps such as intermittent pneumatic compression devices (IPCDs), and compression stockings are not too tight.
- If the surgery time extends more than 2 to 3 hours, consider periodically lowering the legs to the body level.
- Releasing the patient from lithotomy position must be done by two people with slow and smooth movement.
- Ensure both legs are removed and lowered simultaneously while supporting joints to prevent strain on lumbosacral musculature.
- Special care should be given to patients with preexisting conditions such as limited range of motion of the hip, morbidly obese, and lumbar backpain.
Nursing Diagnosis
Following is the list of overall nursing diagnoses related to patient positioning for surgical procedures.
- Impaired comfort
- Impaired transfer ability
- Risk for falls
- Risk for impaired skin integrity
- Risk for impaired tissue integrity
- Risk for perioperative hypothermia
- Impaired physical mobility
- Risk for peripheral neurovascular dysfunction
Documentation tips
- Location and type of padding used (i.e., pillow to support knees or calves, padding under heels)
- Type of stirrups used; including names and roles of persons placing legs in stirrups
- Type of lithotomy position (i.e., low, standard, high, exaggerated, or hemi)
- Presence of distal pulses, color, and temperature of legs and feet
- Use of IPCDs or graduated compression stockings
- Any changes from the preoperative condition should be documented and verbally reported as well.
Conclusion
The lithotomy position is a common position used by clinicians for various examinations and surgical procedures. It has different variations, namely, low, standard, high, exaggerated, and hemi lithotomy position.
However, it is associated with various complications such as peripheral neuropathies and compartment syndrome. So, you must ensure all preventive measures are taken care of in order to prevent complications associated with lithotomy positioning.
Reference
Alexander, E., McEwen, D., & Rothrock, J. (2019). Alexander’s Care of the Patient in Surgery (16th ed.). Elsevier.
Perry, A., Potter, P., & Ostendorf, W. (2014). Clinical nursing skills & techniques (8th ed.). Mosby/Elsevier.
Servant, C., Purkiss, S., & Hughes, J. (2009). Positioning Patients for Surgery. Cambridge University Press.
Timby, B. (2009). Fundamental nursing skills and concepts (9th ed.). Wolters Kluwer Health/Lippincott Williams & Wilkins.

Comments are closed.